

Introduction
Background and Necessity of Research
Purpose and Scope of Research
Research Methodology and Definition of Sustainable Utilization
Methodology
Concepts and Characteristics of Modular Architecture
Defining Standard Dimensions for Modular Medical Units
Concepts and Current Status of Modular Emergency Medical Facilities
Feasibility of Modular Architecture for On-site Emergency Medical Response
Potential for Application 1: On-Site Emergency Medical Response
Potential for Application 2: Infectious Disease Control and Specialized Medical Response
Case Study and Analysis of MEMF
Functional Domain – Purpose of MEMF usage
Functional Domain – Temporal Typology
Spatial Domain – Mobility
Spatial Domain – Scalability/Expandability
Spatial Domain – Circulation System
Technical Domain – Configuration Layout
Technical Domain – Utility System
Deriving Architectural Planning Elements for MEMF Through Case Analysis
Conclusion and Discussion
Summary of Analytical Process and Derivation of Results
Conclusion
Discussion: Future Research Directions and Expected Contributions
Introduction
Background and Necessity of Research
Recent global crises, such as the COVID-19 pandemic and other disasters, have exposed significant vulnerabilities in existing medical systems. These shortcomings highlight the critical need for immediate, on-site emergency response capabilities and underscore the importance of developing rapid and adaptable healthcare infrastructure. In unexpected disasters or emergencies, the ability to rapidly secure sufficient medical space to accommodate patient surges becomes imperative. Modular architecture, characterized by the pre-manufacturing of components in factories for swift assembly at emergency sites, is increasingly recognized as an effective solution for Emergency Medical Facilities (MEMF).
In recent years, there has been a notable increase in the application of modular construction technologies for developing mobile medical facilities, both domestically and internationally. For instance, during the COVID-19 outbreak in Wuhan, China, a modular hospital with over 1,000 beds was constructed in just over ten days, demonstrating the potential for rapid emergency deployment [1]. Similarly, modular wards have been utilized in Korean hospitals designated for infectious disease management.
However, current mobile medical facilities in Korea predominantly rely on tent-type or vehicle-based platforms. These existing models often fail to provide the same spatial quality and medical functionality as permanent hospital buildings. This situation presents two key challenges in emergency response: firstly, the need for platforms suitable for rapid deployment, such as vehicle-based systems; and secondly, the need for platforms adaptable to field conditions, like tents. Modular architecture, with its inherent relocatability and adaptability, offers a promising solution by enabling both rapid and field-responsive construction. Furthermore, modular construction promotes sustainability through material reuse and spatial reconfiguration. Therefore, to establish MEMF that are both mobile and clinically functional, it is crucial to identify and systematize the architectural planning elements that support such development.
Purpose and Scope of Research
The primary objective of this study is to derive the architectural planning elements necessary for establishing MEMF capable of responding swiftly to emergency medical demands in the field. This research investigates the architectural applicability of MEMF and, through an analysis of case studies, identifies key considerations for contemporary mobile modular hospitals. These findings are then synthesized to propose planning elements that foster the sustainable use of MEMF. Ultimately, this study aims to establish a systematic architectural framework applicable to diverse emergency scenarios and to serve as a foundation for practical implementation.
The scope of this study encompasses the following: Functionally, it concentrates on emergency healthcare systems that can rapidly respond to a spectrum of crisis situations, including natural disasters and infectious disease outbreaks. Architecturally, it centers on emergency facilities constructed using modular platforms that support relocation and rapid deployment. The analysis particularly emphasizes steel-frame modular systems, which are dry construction methods offering fast assembly and structural reliability [2]. For empirical analysis, this study surveyed 22 manufacturers of healthcare-related modular architecture and reviewed 27 modular mobile hospital projects. These analyses provide a comprehensive understanding of current modular medical space production and reveal how modular mobile hospitals have been deployed to meet the demands of various disaster and emergency scenarios.
Research Methodology and Definition of Sustainable Utilization
This study employed a literature review as its primary methodology to examine the conceptual foundations of modular architecture and MEMF. A key aspect of this research is to redefine “sustainability” as it pertains to mobile modular hospitals. To assess the feasibility of modular construction as a platform for emergency medical services, case studies of existing facilities were investigated. Based on this analysis, key architectural planning elements were derived from both domestic and international examples of modular medical facilities.
Planning medical facilities involves more than simply placing healthcare programs within enclosed architectural volumes. For modular medical units, operational viability necessitates a careful alignment between the selection of applicable medical programs, the environmental quality of healthcare spaces, and the architectural logic governing system operations. Consequently, the role of architectural planning elements in MEMF is to establish the foundational criteria for rapid deployment and effective operation in future disaster or emergency contexts. These elements are essential to ensure spatial readiness and planning efficiency in response to unpredictable crises.
While the fundamental role of MEMF is rapid response, its architecture must also accommodate uncertainty. Emergency events occur without warning and vary in scale and duration. Therefore, MEMF must be planned with long-term operability in mind. This study interprets “sustainability” not as permanence, but as the capacity for progressive adaptation. Unlike conventional, fixed hospitals, MEMF must respond in phases—initial deployment, adjustment, and expansion— based on how a situation evolves. Sustainability in this context thus refers to the ability to seamlessly expand or combine modular units in response to evolving on-site demands.
Methodology
Concepts and Characteristics of Modular Architecture
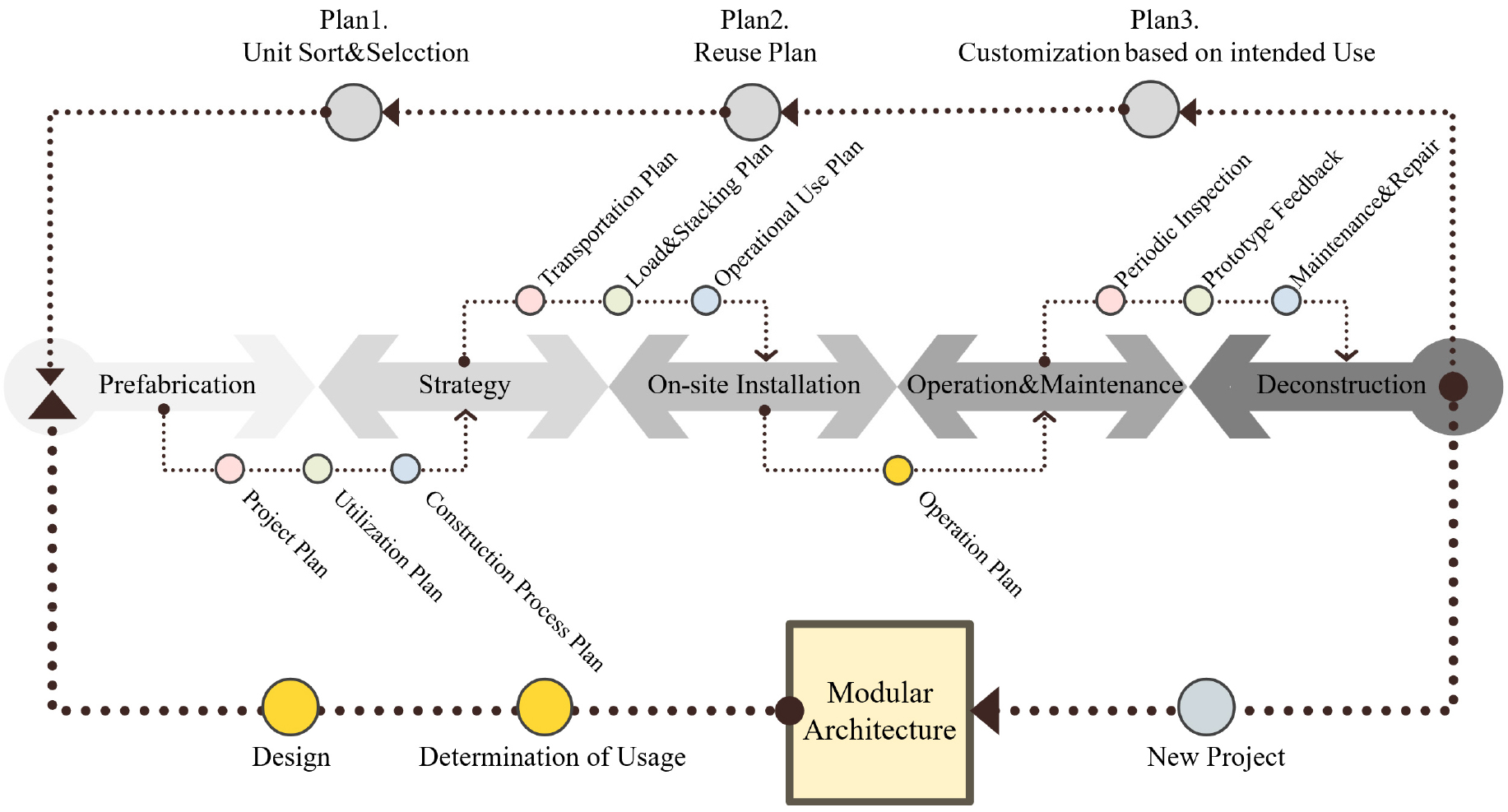
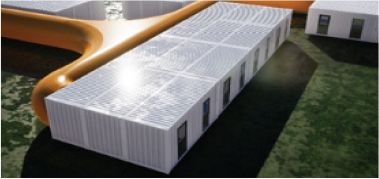
Modular construction is an off-site construction (OSC) method where over 70% of major building components are factory-manufactured, with on-site operations primarily involving assembly and installation [3]. Through standardized members and processes, modular construction enables faster project delivery, ensures higher quality, reduces costs, and minimizes waste. Since units are produced in a controlled environment, uniform quality management is achievable, and weather-related delays are significantly reduced, resulting in construction periods shortened by over 50% compared to conventional methods [4]. Additionally, as illustrated in Figure 1, modular units can be transported and reassembled, offering advantages in recycling and reuse across the building’s life cycle, thereby promoting sustainable use.
Nevertheless, because modular construction involves transporting prefabricated units from the factory to the site, it is subject to transportation standards regulated by laws such as road traffic regulations. These standards impose restrictions on unit dimensions (width, height, and length) [5], which can limit the design and size flexibility of individual units. Furthermore, key technical challenges persist, including joint treatment between units, ensuring structural integrity, and coordinating building utility systems. Research addressing these issues is actively being conducted worldwide [6].
Defining Standard Dimensions for Modular Medical Units
To conduct research on modular construction-based medical spaces, an analysis of actual usable space standards is required. The dimensional specifications of modular medical units are governed by various national and international constraints. This study investigates these constraints based on the context of South Korea to derive feasible unit dimensions. The analysis is based on five primary categories: (1) domestic road traffic laws and standards [7, 8, 9, 10, 11, 12]; (2) vehicle dimension permit regulations [6]; (3) general road conditions [6]; (4) trailer specifications based on ISO container standards [6]; and (5) required medical space dimensions derived from prior research. Within these categories, the study analyzed the viable dimensional range for modular units intended for medical use, as summarized in Table 1. The cited research on transportation limits refers to an analysis of maximum permissible dimensions for oversized cargo under Korean road regulations [13]. Furthermore, preceding studies on medical space focused on the dimensions of an intensive care unit (ICU) bed, which includes the surrounding area required for medical procedures [14, 15, 16].
Table 1.
Analysis of Limiting Factors for Modular Medical Units (Based on outer dimensions)
The analysis concludes that for the Korean context, the feasible dimensions for a modular medical unit are a width of 3.3 m, a height of 3.7 m, and a length ranging from 3.3 m to a maximum of 13.2 m. Although the maximum transportable height in Korea is 4.2 m, a height of 3.7 m was determined as the optimal dimension to ensure stable transport when accounting for the vehicle deck height. The length was planned as a multiple of the width, starting from a minimum of 3.3 m. This design allows for the transport of up to four 3.3 m-long units in a single shipment.
Concepts and Current Status of Modular Emergency Medical Facilities
Modular Emergency Medical Facilities (MEMF) are designed to apply the advantages of modular construction to emergency medical services. They aim to deliver complete medical spaces rapidly during unpredictable crises, such as emergencies, disasters, and pandemics. MEMF is increasingly recognized as a viable alternative that addresses the physical expansion constraints of fixed healthcare facilities and the limited functionality and durability of conventional mobile healthcare platforms like tents and vehicle- based units [6]. By assembling standardized medical units, MEMF can accommodate diverse emergency medical programs—including patient triage, treatment, surgery, and inpatient care—within a single modular system [17].
The ability to relocate and reconfigure individual spaces allows MEMF to be quickly deployed in disaster zones, remote areas, and existing hospital sites. It also offers scalability, enabling easy expansion or downsizing according to situational demands. Moreover, MEMF can maintain building-quality environments, including structural safety and integrated utility systems (e.g., negative-pressure and air-conditioning), making it capable of supporting high-level medical care requirements such as infectious disease management and critical patient treatment.
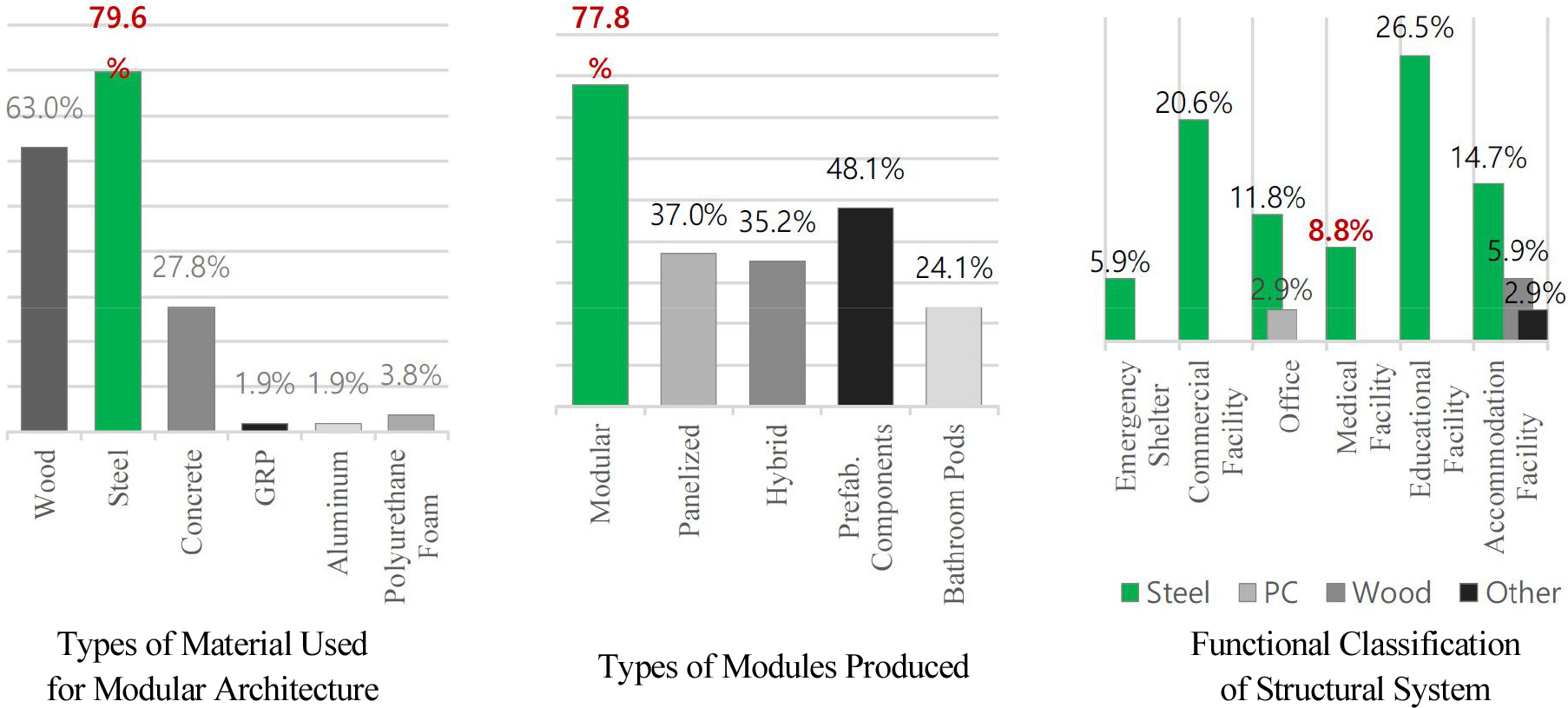
As the global need for MEMF increases, technological advancements and pilot projects are being actively pursued. The COVID-19 pandemic, in particular, spurred intensive research into MEMF applications like negative-pressure isolation wards and screening stations [18]. Furthermore, major international organizations, including the UN and WHO, now offer standardized guidelines for modular healthcare facilities designed for disaster response [19, 20, 21, 22]. In addition, modular construction has demonstrated its practical applicability and is now actively utilized as medical space both domestically and internationally. As shown in Figure 2, a survey in the United States indicates that steel-frame modular construction is the most widely used method for medical applications [23, 24]. However, standardized classification criteria for production methods, functions, and quality are still lacking, hindering efficient utilization and broader adoption.
Feasibility of Modular Architecture for On-site Emergency Medical Response
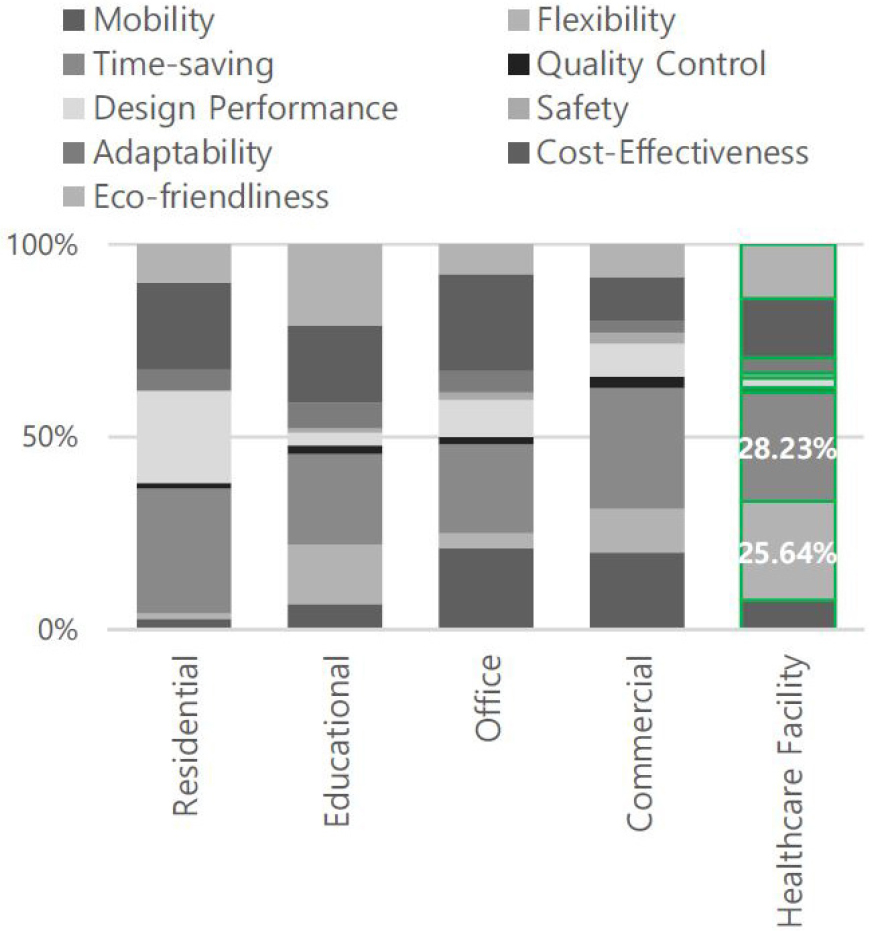
The feasibility of applying modular construction to healthcare facilities can be assessed by examining the significance of its characteristics. A previous study termed these characteristics ‘success factors,’ explaining them as elements necessary to meet client demands or reasons for choosing modular construction for specific building types [25]. This study classified modular building types into residential, educational, office, hospital, and commercial facilities, identifying key success factors for each. These key success factors also represent distinctive features and are summarized in Table 2.
Table 2.
Key Features and Success Factors of Modular Architecture Applicable to MEMF
As depicted in Figure 3, the analysis revealed that for hospital facilities, the most crucial success factors were flexibility, shortened construction time, and economic efficiency, in that order [25]. This finding corroborates the earlier discussion that MEMF must offer flexible space usage responsive to the unpredictable needs of an emergency site. The ability to shorten construction schedules is also critical, as rapid on-site deployment is essential for emergency medical facilities. Furthermore, because MEMF can be reused and relocated, economic efficiency becomes a significant advantage.
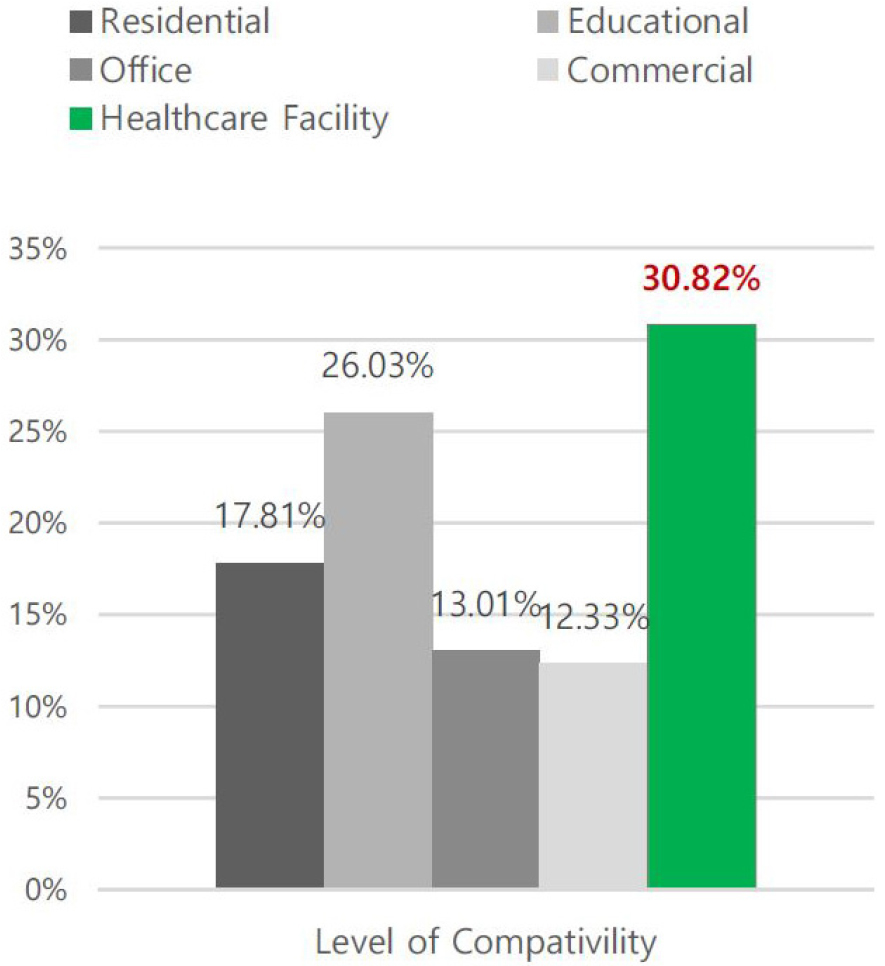
Based on the success factors identified in previous studies, a further analysis was conducted to evaluate the suitability of modular construction for different building types. As shown in Figure 4, healthcare facilities accounted for the highest proportion at 30.82%, followed by educational and residential facilities [25]. This suggests a high compatibility between healthcare facilities and modular construction, particularly because modular systems enable quick unit combinations, easy spatial adjustment based on needs, and high economic sustainability through reuse.
Potential for Application 1: On-Site Emergency Medical Response
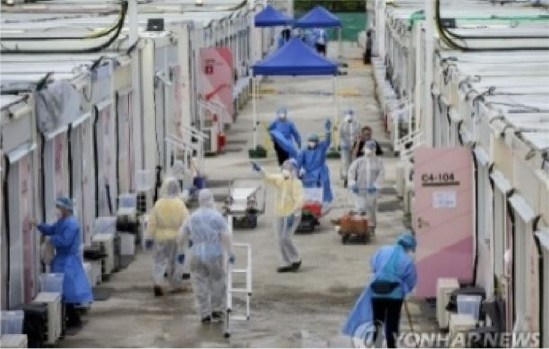
Emergency events occur unpredictably, making rapid medical response and the immediate securing of on-site medical space critical. In large-scale disasters or natural catastrophes, Disaster Medical Assistance Teams (DMATs) are dispatched, and on-site emergency medical posts are established to deliver initial care. However, as summarized in Table 3[26, 27, 28, 29, 30, 31], such facilities—both in Korea and abroad—often rely on portions of nearby buildings or temporary structures like tents, resulting in limited space and restricted medical capacity. In Korea, on-site emergency medical posts operate under the 3T framework (Triage, Treatment, Transport), yet resource and facility constraints limit further medical interventions. Nevertheless, these posts are vital for interventions within the “golden hour,” and their increasing deployment numbers highlight their importance.
Table 3.
Case of On-site Emergency Medical Posts / DMAT Emergency Response
 |  |  |
| Barbados / Field Operation | UK / Field Operation | Korea / On-site mobile Clinic |
 |  |  |
| Korea / DMAT Response | Korea / On-site mobile Clinic | Korea / Field Operation |
With the prolonged nature of disasters, the necessity for mobile modular hospitals has gained greater attention. Manuals and operational guidelines, such as those from the Carolina mobile modular hospital project in the United States, have been established, with modular construction commonly serving as the underlying system. This reflects the significant potential of modular construction as a platform for emergency medical responses. Today, national and international organizations, including Korea’s Disaster Emergency Medical Manual and the WHO Field Operation Manual, propose modular approaches for emergency healthcare infrastructure.
Despite this, clear standards for unit-specific medical programs, integrated facility systems, and unit combination methods are still lacking. Furthermore, there is a shortage of detailed architectural discussions regarding critical aspects such as setup time, spatial requirements, and modular connectivity for emergency facilities. Thus, systematic research is needed to establish planning and construction strategies for MEMF, based on existing guidelines and operational cases. Defining proper specifications for unit and facility dimensions, service environments, and applicable medical programs is essential. Ultimately, MEMF should be positioned not as temporary shelters but as fully realized modular building solutions capable of effectively supporting urgent medical responses.
Potential for Application 2: Infectious Disease Control and Specialized Medical Response
MEMF plays a crucial role in securing isolation facilities during infectious disease outbreaks. Modular units equipped with negative-pressure systems, anterooms, and independent HVAC systems can be rapidly installed, effectively isolating patients and reducing cross-infection risks. The widespread use of modular negative-pressure wards during the COVID-19 pandemic highlighted this strength. Additionally, modular construction can quickly establish screening clinics, testing centers, and vaccination sites as needed.
The COVID-19 pandemic demonstrated that fixed medical facilities alone are insufficient for large-scale infectious disease responses. While early interventions such as screening centers and temporary wards (as shown in Table 4[32, 33, 34]) provided some immediate relief, they were inadequate to fully address infection spread and medical system overload.
Table 4.
Cases of Screening Centers & Temporary Wards


MEMF offers a distinct advantage by enabling fast construction and scalable expansion of infection- specific facilities, such as isolation wards and negative- pressure clinics. Post-pandemic, modular solutions like foldable clinics and mobile screening stations have been deployed globally, reinforcing the value of flexible medical space in public health crises. Moreover, MEMF is increasingly considered in other specialized fields, including mental health emergencies and maternity care in underserved regions, demonstrating its broader applicability. Specifically, modular Mental Health Crisis Units and mobile obstetric clinics have been proposed to meet emerging healthcare demands. Modular construction’s ability to deliver full healthcare functionality within compact, adaptable spaces supports these initiatives.
Looking forward, specialized modular units for trauma care, burn treatment, or cardiovascular emergencies could be developed. Prefabricating specialized units equipped with appropriate medical technologies would enable faster deployment and improve access to critical care services. In this manner, MEMF is evolving from a temporary solution to a sustainable strategy for infectious disease control and specialized emergency healthcare delivery.
Case Study and Analysis of MEMF
To effectively plan and utilize MEMF, it is necessary to assess current applications of modular construction- based medical spaces both domestically and internationally. Additionally, a systematic typological classification is required for a comprehensive analysis of their use. Based on existing research and case analyses, MEMF can be classified into three primary domains: functional, spatial, and technical. Each domain has been examined through representative examples that have been implemented or manufactured in practice [6]. The case studies on modular construction-based medical units were conducted by reviewing information provided through official company websites, product catalogs, and publicly distributed materials.
The Functional Domain focuses on how MEMF are utilized in different emergency contexts, assessing their purpose and deployment conditions. It also investigates the timeframes required for installation, aiming to evaluate the functional appropriateness of current MEMF implementations and their effectiveness in supporting emergency medical operations. Excluding functional aspects, MEMF—when viewed purely in physical terms—does not differ substantially from typical steel-frame construction.
Thus, the Spatial Domain investigates characteristics intrinsic to the modular unit: mobility, scalability, interconnectivity, and circulation systems. This analysis enables the identification of spatial features pursued by current mobile hospitals and reveals how different medical programs are physically arranged and interrelated. The purpose of this investigation is not only to examine how space serves immediate medical functions but also to explore how spatial solutions can support the sustainable use of MEMF over time.
The Technical Domain addresses characteristics specific to modular construction, including unit configuration layouts and the implementation of building service (utility) systems. As MEMF are composed of discrete modular units, each performing a specific medical function, the analysis focuses on how environmental requirements—particularly utility systems—are applied to support individual units and how circulation infrastructure is integrated across them. These findings provide insight into the environmental strategies necessary for MEMF to function as effective healthcare facilities.
Functional Domain – Purpose of MEMF usage
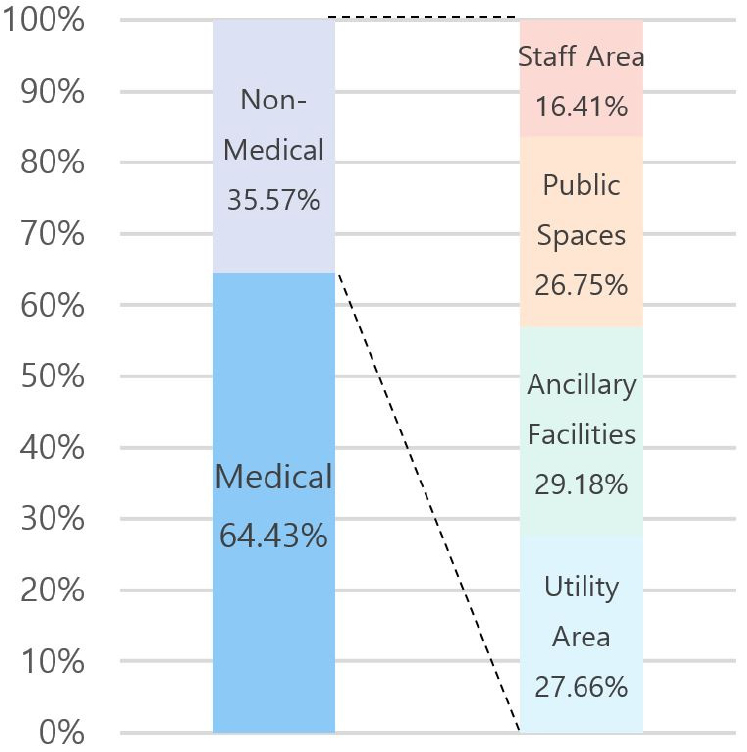
MEMF are composed of a combination of clinical and support programs, similar to conventional fixed healthcare buildings. Medical units perform primary healthcare services, while non-medical units support them through logistical and environmental functions. Non-medical programs—referred to as support units—include utility infrastructure, auxiliary spaces, public spaces, and staff-related zones. Corridor units are particularly essential to MEMF layout, providing core access areas (e.g., vestibules and airlocks) and acting as key distribution routes for mechanical and electrical systems.
According to the analysis (Table 5), 35.57% of modular units serve non-medical functions, while 65.43% are medical units directly involved in treatment or care delivery. These functions are closely linked operationally. Among modular units currently in production or actual use, medical-purpose units are more widely manufactured and show higher deployment levels.
Table 5.
Utilization Rate of MEMF by Purpose of usage: A Case Study Analysis



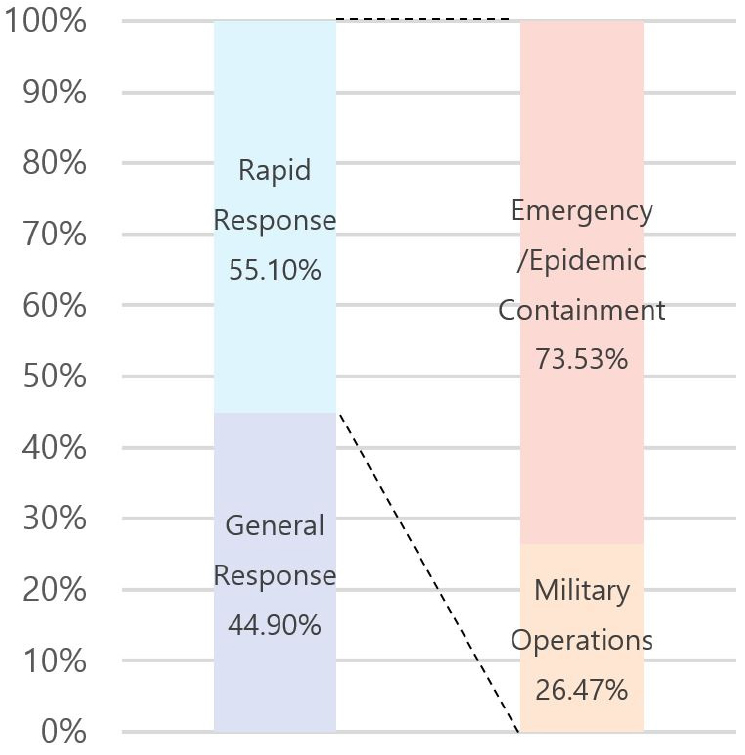
Functional Domain – Temporal Typology
Modular construction platforms for mobile hospitals offer a strategic architectural response to emergencies that trigger sudden spikes in healthcare demand, such as national disasters, pandemics, and large-scale public events. Owing to their unitized and prefabricated nature, MEMF can also be integrated into existing hospital campuses as extensions or supplementary structures. Each physically uniform unit can accommodate a wide range of medical programs based on differing objectives and usage contexts, allowing the same spatial volume to serve distinct healthcare functions.
MEMF is therefore not limited to disaster response. It can also serve as a rapidly deployable facility for military operations or exhibitions, or function as temporary support space during the expansion or renovation of general healthcare institutions. These varied use cases reflect different temporal expectations and levels of urgency, forming the basis for classifying MEMF into two main categories: rapid-response and general-response. The rapid-response type is designed for high-urgency contexts such as military operations, emergency relief, and epidemic containment. In contrast, the general-response type is typically used in general healthcare functions—for example, as interim clinics during hospital reconstruction or as semi- permanent facilities to expand healthcare coverage. This classification framework clarifies that MEMF extends beyond emergency care; as it becomes more embedded in general healthcare systems, its role as a flexible and sustainable architectural solution is further reinforced. Case data (Table 6) show that 55.1% of facilities were designed for rapid-response, while 44.9% were for general-response use, highlighting the broad functional adaptability of MEMF across both emergency and non-emergency scenarios.
Table 6.
Utilization Rate of MEMF by Temporal Typology: A Case Study Analysis

Spatial Domain – Mobility
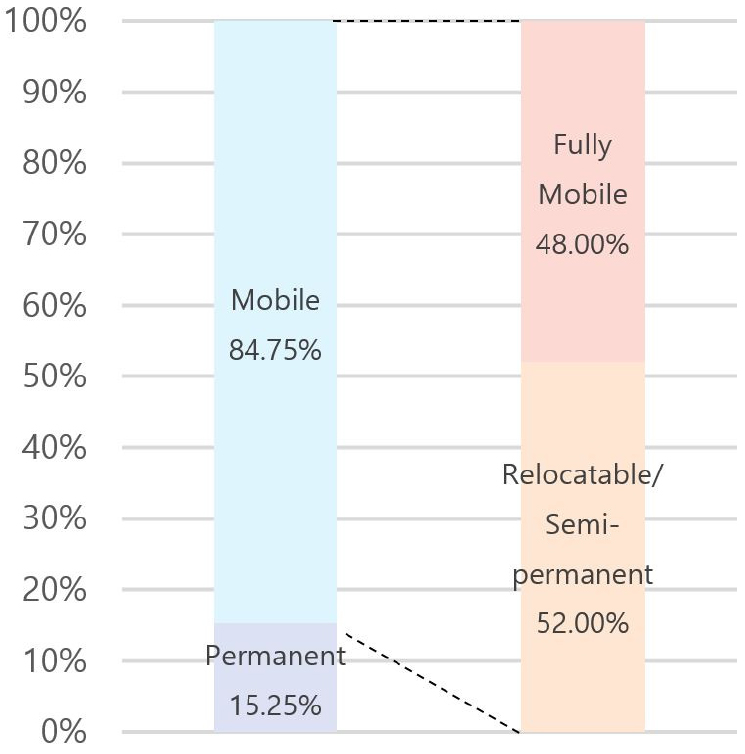
MEMF can be categorized by mobility into three types: mobile, relocatable, and permanent. Mobile MEMF are characterized by ease of installation and dismantling, making them highly suitable for urgent and temporary deployment in emergency situations. Relocatable MEMF are based on mobile configurations but are structurally reinforced for longer-term use, offering enhanced stability suitable for multifunctional applications like infection control and clinical treatment. Permanent MEMF, conversely, are designed as permanent healthcare structures, not considering future relocation or reuse, and function as complete, stationary medical facilities. This classification reflects how MEMF can be adapted to different operational contexts depending on the required mobility and duration of use, particularly suiting emergency response scenarios where rapid deployment and relocation are critical. Overall case analysis (Table 7) indicates that approximately 85% of MEMF fall under the mobile or relocatable category, demonstrating that mobility—a core characteristic of modular architecture—is widely adopted in modular healthcare applications.
Table 7.
Utilization Rate of MEMF by Mobility: A Case Study Analysis



Spatial Domain – Scalability/Expandability
The scalability of modular construction-based healthcare facilities refers to their capacity to flexibly respond to changes in spatial requirements or additional functional demands post-installation. For MEMF, scalability is categorized into three types (Table 8): Optimal Expandable, self-expandable, and unit combined expandable. Unit combined expansion involves structurally combining new modular units with existing ones to increase usable area or enhance functional capacity, proving particularly effective for rapid facility expansion under emergency conditions. In contrast, self-expansion involves units inherently designed for on-site extension without adding new modules; these require structurally reinforced configurations and are often used in military operations, infection control, and field-based care due to their adaptability and stability. Optimal expansion describes units initially produced as complete facilities that can later be extended by adding equipment zones or specialized rooms, allowing for future upgrades and long-term flexibility in medical service delivery.
Table 8.
Utilization Rate of MEMF by Scalability/Expandability: A Case Study Analysis
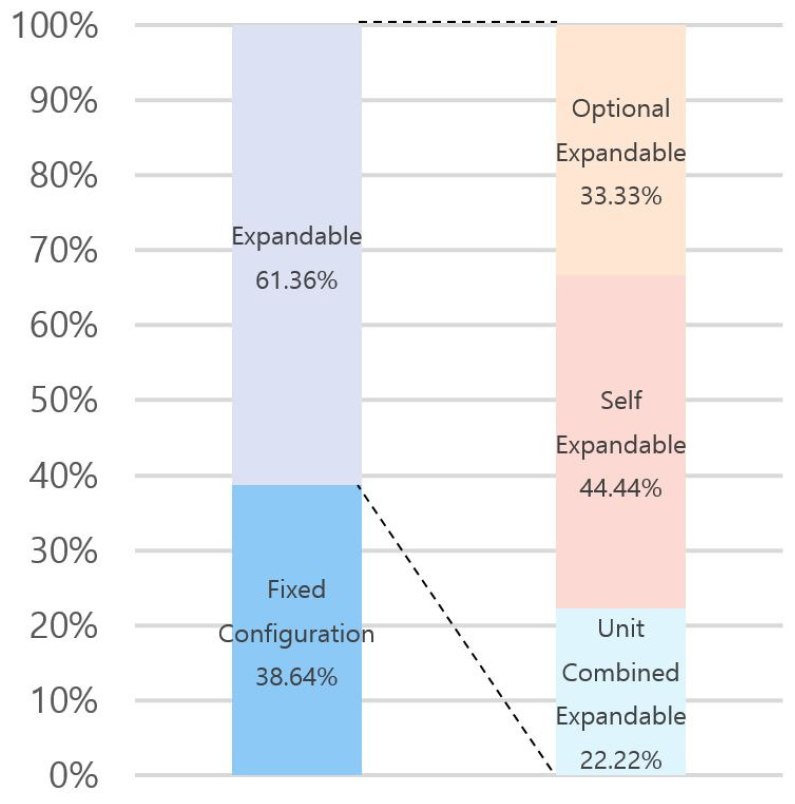


Case analysis shows that modular units are nearly evenly divided between expandable (44.44%) and fixed configuration (45.56%) types. Among expandable cases, self-expandable units account for 75.0%, indicating a strong preference for internally scalable modules. These findings suggest that MEMF is not only a rapidly deployable system but also a spatially adaptable one, capable of addressing both immediate medical needs and longer-term infrastructure planning.
Spatial Domain – Circulation System
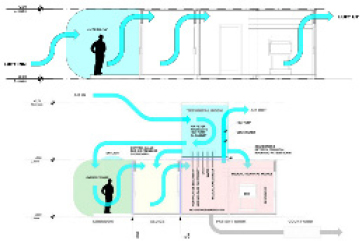
As shown in Table 9, MEMF circulation systems can be categorized into two primary typologies based on the spatial configuration and directional relationship between circulation paths and unit layout: single-loaded corridor and double-loaded corridor. A hybrid configuration combining both types may also be applied, depending on programmatic complexity. The circulation system critically influences spatial efficiency and functional performance, directly impacting unit arrangement and corridor utilization; therefore, it must be carefully planned in alignment with the facility’s scale and operational goals.
Table 9.
Utilization Rate of MEMF by Circulation System: A Case Study Analysis
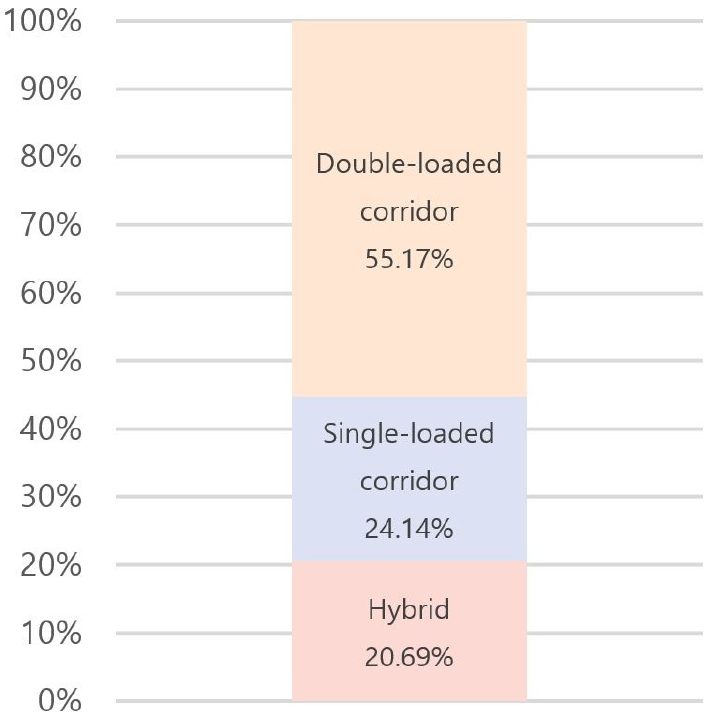
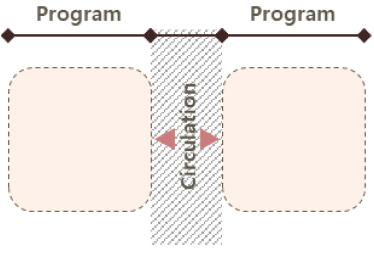
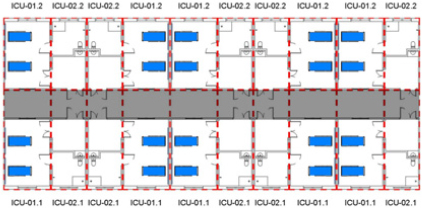
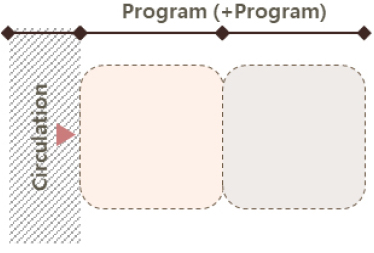
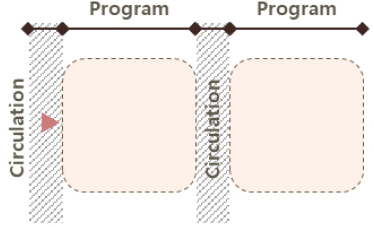

The single-loaded corridor configuration features a linear layout with units aligned along one side of a corridor, typically based on the unit’s short side (end wall), though it can also be organized along the long side depending on spatial constraints. Due to its simplicity, it is most often used in smaller-scale facilities. In contrast, the double-loaded corridor configuration places modular units on both sides of a central corridor, using either the short or long axis of the unit. In the short-axis version, units are placed on both sides of the corridor with their end walls facing the center; in the long-axis version, the longer sides of the units line the corridor. This layout offers advantages in land efficiency, circulation clarity, and separation between functional and transitional zones. Consequently, the double-loaded corridor configuration is found in approximately 55% of analyzed MEMF cases, making it the most frequently adopted system. It is considered particularly well-suited for temporary emergency medical facilities like MEMF, where rapid and high-efficiency spatial deployment is critical. Lastly, the hybrid configuration, combining single- and double-loaded corridor types, may be applied in larger facilities requiring a more complex arrangement of medical programs, though it is less common due to planning complexity and resource demands.
Technical Domain – Configuration Layout
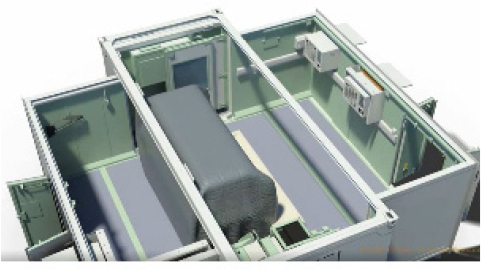
The configuration layout of MEMF can be broadly categorized into standalone and integrated response types (Table 10), depending on whether modular units operate independently or are structurally connected. This classification is fundamentally based on the presence or absence of unit-to-unit linkage, which significantly influences the facility’s scale, flexibility, and service scope.
Table 10.
Case Studies for Configuration Layout of Modular Healthcare Facilities





Standalone configurations consist of a single modular unit designed for autonomous function. These units are suitable for rapid deployment in emergency scenarios requiring immediate but limited medical support, such as basic treatment or primary care. Their compact footprint and fast installation allow for quick response in field conditions. However, standalone units have inherent limitations in spatial expansion and functional diversity, making them less suitable for long-term or multifaceted healthcare services.
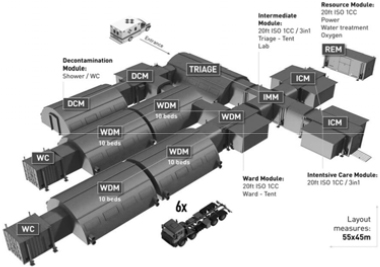
In contrast, integrated configurations comprise multiple modular units physically connected to form a cohesive medical facility. Each unit typically accommodates a distinct medical function—such as triage, diagnostics, treatment, or isolation—and together they form a unified system capable of delivering comprehensive healthcare services. These configurations are planned according to specific site conditions and medical requirements, enabling flexible adaptation to both small- scale and large-scale operations. Notably, integrated layouts allow for spatial growth and programmatic layering, supporting the development of multi-unit or even multi-story modular healthcare infrastructures. By enabling either minimal or comprehensive medical service delivery, this configuration strategy underscores the scalability and adaptability of MEMF across various deployment contexts—from single-unit emergency responses to complex, mission-driven modular hospitals.
Technical Domain – Utility System
Based on case study results, MEMF utility system configurations can be classified into three types (Table 11): external utility units, built-in systems, and portable systems. Each configuration exhibits distinct characteristics depending on facility scale, operational context, and medical response strategy.
Table 11.
Utilization Rate of MEMF by Utility System: A Case Study Analysis
| Category | Content | Category | Content |
| Utility System | 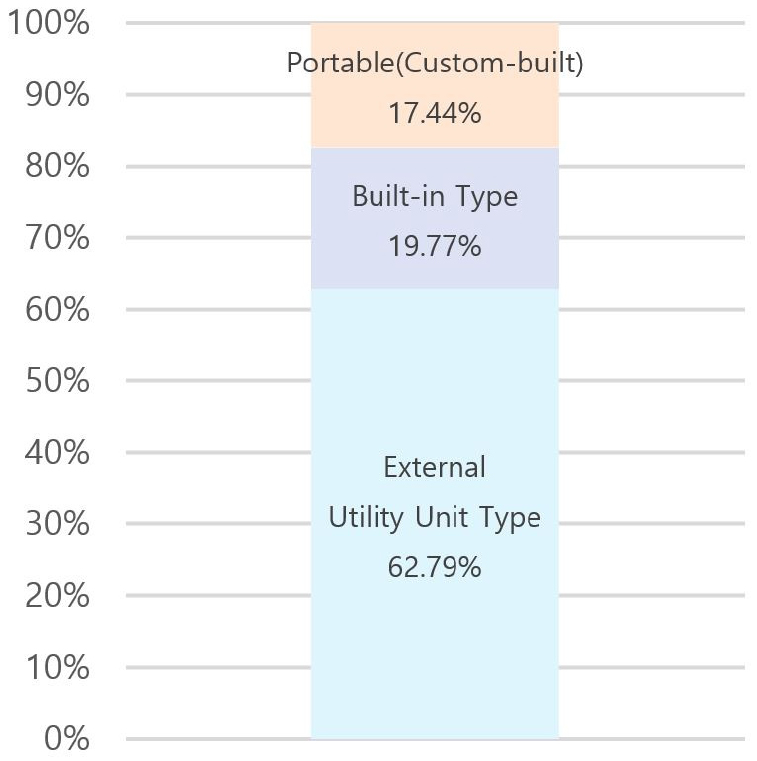 |
Portable (Custom-built) |  |
| Internal Type |  | ||
|
External Utility Unit Type |  |
The external utility unit type accounts for the majority of cases (62.79%), most commonly applied in emergency medical environments where multiple modular units require centralized utility coordination. Its primary advantage lies in supporting a wide range of medical functions through shared infrastructure and expanded service capacity. The built-in system, embedding utilities within a single modular unit, offers self-sufficient operation and is more suitable for standalone unit deployments. Although its service scope is limited by unit capacity, it provides operational independence and faster installation. The portable utility system represents a small-scale, mobile solution flexibly deployed with single units or small clusters, particularly useful in field conditions requiring lightweight infrastructure or rapid relocation.
The external utility unit model is especially effective for facilities requiring coordinated operation among multiple medical modules, where centralized systems enhance performance through integrated service provision. Nevertheless, in high-risk or isolated contexts—such as disaster zones or infectious disease containment sites—complete reliance on externally supplied utilities may not be feasible. Therefore, a hybrid planning strategy is recommended: while external utility units should form the system’s central backbone, built-in and portable systems should be incorporated in parallel to ensure operational independence where required. These findings highlight the importance of tailoring infrastructure planning to the deployment context. In designing modular medical units, the characteristics, strengths, and limitations of each utility configuration must be considered. Prioritizing external utility units while integrating built-in and portable solutions for site-specific resilience can achieve a more flexible and adaptive infrastructure, capable of supporting diverse healthcare environments under both normal and extreme conditions.
Deriving Architectural Planning Elements for MEMF Through Case Analysis
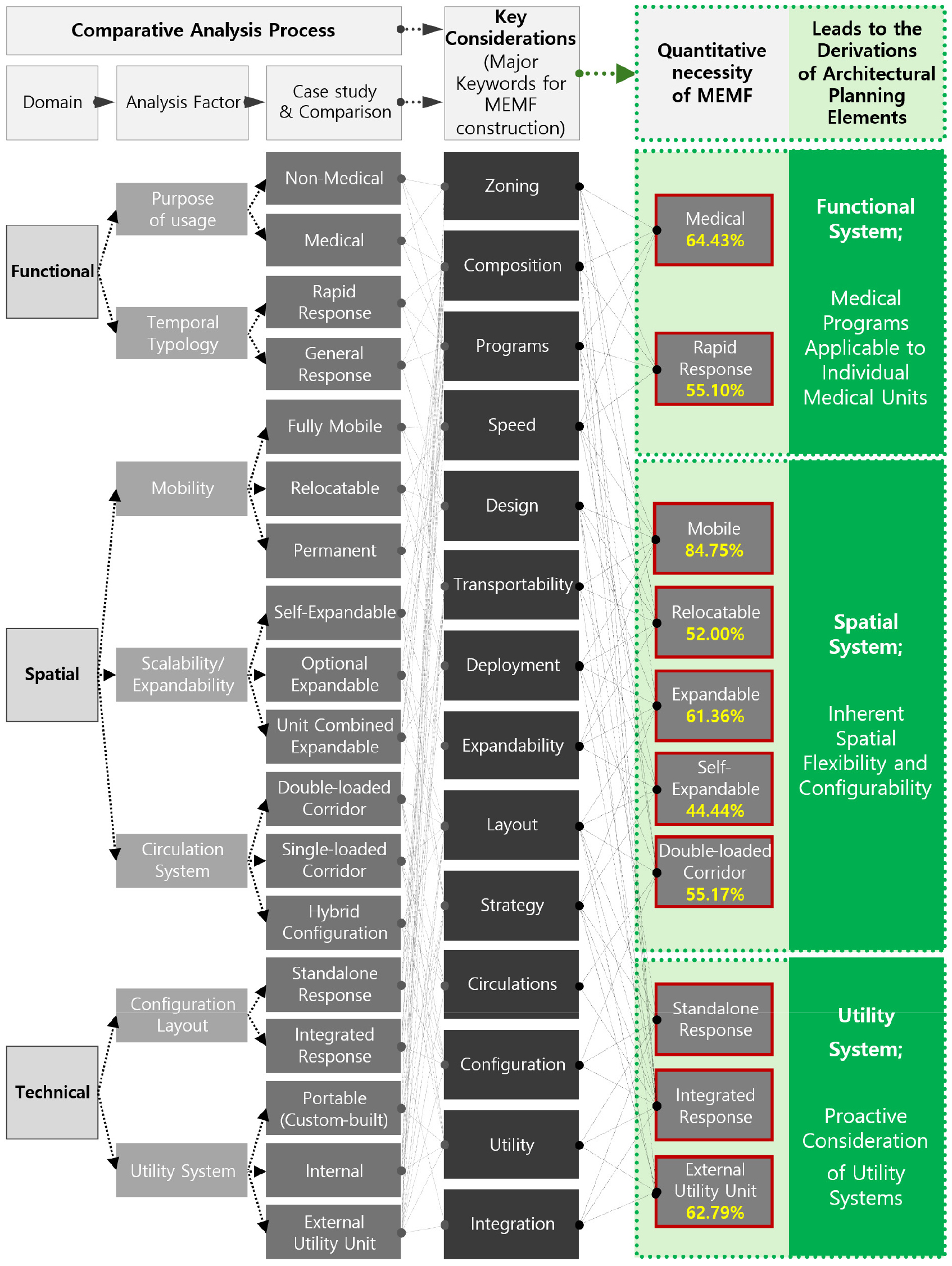
The functional, spatial, and technical characteristics observed in MEMF case studies are summarized in Table 12, illustrating the analytical process leading to the derivation of architectural planning elements (Figure 5). This table encapsulates prior case analyses, mapping how they inform and validate the proposed planning framework for MEMF. Importantly, the three initial classification domains—function, space, and technology—were found to align with and complement the final set of planning elements. This suggests that both past and current MEMF implementations have incorporated these elements, either explicitly or implicitly, into their design and deployment. These findings underscore the relevance of modular construction features and the operational requirements of mobile medical facilities, providing a foundation for future technological refinement and strategic MEMF deployment planning.
Table 12.
Derivation of Architectural Planning Elements for MEMF Based on Case Study Analysis
Regarding unit function, approximately 60% of modular units were classified as medical, with the remaining 40% associated with non-medical support functions. These non-medical units primarily sustain clinical operations by providing utilities, circulation space, staff areas, or auxiliary functions. The coexistence and spatial integration of medical and non-medical units in MEMF indicate that healthcare delivery in such facilities relies not only on treatment spaces but also on an appropriately planned support infrastructure; thus, coordinated spatial planning reflecting both categories is essential.
When analyzed by temporal deployment type, emergency-response applications were more prevalent than general-response applications. This trend underscores the appropriateness of modular construction in urgent healthcare scenarios, such as disaster relief, epidemic response, or military operations. The findings support the conclusion that modular healthcare facilities are structurally and operationally aligned with the rapid-response requirements of emergency medicine.
From a mobility perspective, approximately 70% of analyzed units were found to be relocatable. This result reinforces the importance of modularity’s inherent flexibility in field-based medical environments where quick setup, disassembly, and redeployment are critical. The predominance of mobile applications confirms that MEMF are particularly well-suited to dynamic or temporary medical contexts.
In terms of scalability, the analysis suggests that the critical determinant is not simply whether a unit is expandable, but rather how expansion is realized—either through combining multiple modules or using structurally expandable single units. These planning decisions varied depending on user preferences, manufacturers’ production capacity, and specific site demands. Importantly, ongoing advances in modular production technologies have enabled diverse approaches to achieving scalable space without sacrificing performance or medical functionality.
The circulation system analysis compared MEMF layouts with standard healthcare circulation typologies, finding that rational, efficiency-driven systems, such as the double-loaded corridor layout, were prioritized over aesthetic concerns. Particularly for facilities designed for rapid emergency deployment, functional clarity and operational efficiency were identified as the primary drivers of spatial planning. Approximately 55% of the facilities adopted double- loaded corridor configurations, confirming its prevalence and appropriateness for MEMF.
Regarding facility configuration, layouts were categorized as either standalone or integrated, depending on whether units function independently or are structurally combined. This classification was not dictated by standard usage patterns but by the nature of the medical programs being delivered. As such, the configuration type was determined by whether site conditions and clinical goals required a single-unit operation or a multi-unit composite system.
In the technical domain, utility system configurations were found to be of three types: external utility units, built-in systems, and portable systems. The analysis revealed that external utility units were used approximately 40% more frequently than other types, reflecting a strong preference for centralized utility management across multiple modules. However, for settings demanding infrastructure self-sufficiency—such as disaster zones or infectious disease control sites—the combined use of built-in or portable systems becomes essential. Hybrid approaches integrating multiple utility strategies were found to increase adaptability in highly variable field conditions.
As a result of systematic case analysis, this study identifies key architectural planning elements that must be considered for the sustainable application of MEMF. The analysis, structured around three domains—functional, infrastructural, and spatial—along with seven detailed criteria, reveals three core planning imperatives:
•Pre-defining medical programs based on the integrated coordination of healthcare and auxiliary service units.
•Anticipating technical elements for utility systems and environmental control suited to medical practices.
•Accommodating spatial flexibility for modular unit- based configuration.
These three domains define the architectural foundation upon which Modular Emergency Medical Facilities (MEMF) can be effectively realized, deployed, and maintained across diverse emergency healthcare environments.
Conclusion and Discussion
Summary of Analytical Process and Derivation of Results
This study aimed to derive essential architectural planning elements for Modular Emergency Medical Facilities (MEMF), which are designed for direct and effective on-site responses during urgent medical demands. The research began with a comprehensive literature review to establish conceptual definitions for modular architecture and MEMF. This review also examined the current status and feasibility of applying modular architectural systems to emergency medical scenarios. Following this, an in-depth case study analysis was conducted, covering 22 domestic and international manufacturers of healthcare-related modular medical facilities and 27 mobile hospital projects.
This empirical investigation involved classifying and analyzing existing MEMF applications across three primary domains: functional (including purpose of use and temporal typology), spatial (encompassing mobility, scalability, and circulation systems), and technical (covering deployment layouts and utility systems). The analytical focus was twofold: first, to identify the current capabilities of mobile hospitals that utilize modular architecture, and second, to determine the key architectural elements necessary to ensure their practical on-site responsiveness. Through this systematic and multi-faceted analytical approach, which incorporated typological classification and a comparative review of diverse operational cases, the main characteristics and prevailing trends of MEMF were identified. These findings then directly informed the process of abstracting and systematizing the core architectural planning elements that are crucial for the sustainable and efficient deployment of MEMF.
Conclusion
•The comprehensive analysis undertaken in this study was intended to provide direction for the foundational architectural planning of robust and adaptable MEMF. This process culminated in the identification of essential architectural planning elements. These elements are pivotal in ensuring that modular facilities can be effectively deployed, operated, and maintained within diverse emergency medical environments. Through an integrative study of both qualitative and quantitative analyses, this research synthesizes these multifaceted considerations into three core architectural planning elements (principles).
•The case study methodology in this research serves to represent the macroscopic frequency of demand for MEMF features internationally. In this context, the dominant trends identified within each domain of the qualitative case analysis are interpreted as expressing a quantitative necessity proportional to their prevalence. Thus, these findings effectively represent the quantitative requirements for MEMF, and the overall research conclusions were reached by translating these detailed considerations from each analysis domain into the final architectural planning elements. Here are the research conclusions regarding the three main architectural planning elements for MEMF construction, derived through an integrated research analysis process.
①Strategic Definition of Medical Programs Applicable to Individual Medical Units: This element, derived from the functional analysis of case studies, involves the integrated coordination of primary medical service units with essential auxiliary and support units. Effective MEMF planning requires a clear, upfront understanding and specification of medical functions. This ensures that the modular layout can support seamless operational flows between clinical spaces and logistical support areas, including utilities, staff zones, and circulation pathways.
②Inherent Spatial Flexibility and Configurability: This principle highlights the necessity of designing MEMF with inherent spatial adaptability to accommodate various configurations based on medical units. The architectural planning of MEMF must leverage flexibility—a core advantage of modular architectural spatial composition. This involves allowing for the expansion or reduction of facility scale (scalability), relocatability, and diverse internal layouts to effectively respond to changing on-site demands, different medical scenarios, and varying site constraints. Furthermore, the spatial scale of each unit must be based on its suitability for the intended medical procedures; this requires a prior assessment of scale to accommodate a range of interventions, from simple treatments to advanced medical procedures. Such spatial planning elements extend beyond merely placing specific medical programs in certain locations; they must also comprehensively consider the characteristics of the entire facility, the flow of medical procedures, user circulation, and potential directions for expansion.
③Proactive Consideration of Utility Systems: This element emphasizes the anticipation and integration of appropriate technical systems, particularly concerning utility systems (such as power, water, waste, medical gases, and HVAC) and environmental control systems (like HVAC, pressure control capabilities, and air filtration). Because emergency responses often necessitate the combined operation of multiple medical units rather than a single one, the utility systems in MEMF significantly influence not only the realization of a technical medical environment but also the overall facility layout, program linkage, and user circulation flow. Utility planning must therefore accommodate the specific technical requirements of medical procedures to ensure safe, controlled, and complete functional performance within each medical facility unit.
These three planning elements—programmatic definition, facility system planning, and spatial flexibility—collectively constitute the fundamental architectural framework. Adherence to these planning elements will enable the realization of MEMF that are not only rapidly deployable but also operationally efficient, clinically effective, and sustainable throughout their intended lifecycle when responding to unpredictable crises.
Discussion: Future Research Directions and Expected Contributions
While this study presents a fundamental architectural framework for the planning of Modular Emergency Medical Facilities (MEMF), continuous future research is necessary to expand the practical applicability of this field. In particular, further in-depth research based on the planning elements derived in this study is required in the following directions:
First, from a functional perspective, there is a need to establish specific medical standards aligned with the phased nature of emergency situation responses. Existing emergency medical manuals are predominantly based on guidelines for the construction of temporary spaces such as vehicle-based or tent-type structures. However, while these manuals acknowledge the potential utility of modular construction, specific guidelines that reflect its unique characteristics are currently non-existent. Furthermore, there is a deficiency in guidelines from an architectural planning perspective for emergency response mobile hospitals themselves. Therefore, research is required on phased response guidelines for the construction of medical facilities utilizing modular architecture, which stands as the most realistic platform for the implementation of medical spaces.
Second, from a spatial perspective, validation of MEMF deployment methods and the appropriateness of their scale is required through the implementation of practical pilot projects. Building on the findings of this study, future research should involve conducting simulations within a physical MEMF environment based on established medical scenarios. This process is required to validate the real-world feasibility and applicability of mobile hospitals during emergencies. Validation through simulation extends beyond mere architectural review; it allows for a multifaceted assessment, including the confirmation of necessary medical programs for emergency response, the appropriateness of the overall facility scale, and the identification of environmental components required for specific medical functions. Furthermore, these simulations would provide an ideal opportunity to conduct expert surveys on the architectural planning elements that were qualitatively analyzed in this study. Through this process, quantitative evidence can be established, enabling the derivation of more specific, evidence-based, and definitive architectural planning elements.
Third, from a facility system perspective, a technical analysis of the feasible scope of facility system application within the limited specifications inherent to modular construction is necessary. Globally, modular construction faces dimensional limitations imposed by traffic laws and transportation regulations. Consequently, an analysis of the required facility system levels for performing a certain standard of medical procedures, alongside their physical applicability, would enable the systematic classification and application of MEMF facility levels deployed according to the specific conditions of an emergency site. Such classification is deemed essential.
The anticipated impacts of such research and future endeavors are multifaceted. Primarily, the aim is to enhance societal resilience and preparedness for public health emergencies and disasters by providing a robust framework for the construction and operation of rapidly deployable and effective medical facilities. This can lead to improved patient outcomes, a reduction in the strain placed on existing healthcare systems during crises, and more efficient utilization of resources. Ultimately, by promoting a systematic approach to MEMF design, this line of research will contribute to the broader adoption of modular construction in specialized medical fields and serve as a catalyst for a future paradigm shift in healthcare architecture.
